Our Findings
Frequently monitored biomarkers are not top predictors for cardiac disease in our analysis.
These four common biomarkers are routinely monitored by physicians. However, they did not emerge from our models as top predictors for Major Adverse Cardiac Event (MACE) for neither males nor females.
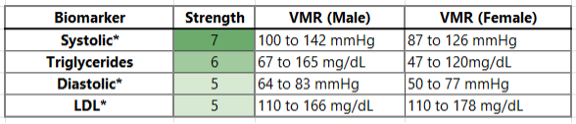
*Individuals are removed from our analysis if they report taking medications intended to directly modify the biomarker, including statins for cholesterol, or anti-hypertensives for blood pressure.
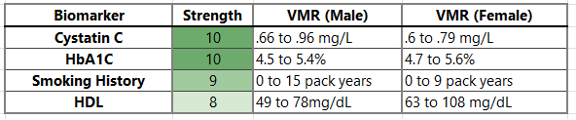
For comparison, below are the most predictive biomarkers in our model inputs for MACE:
Cystatin C is one of the most predictive markers for several diseases.
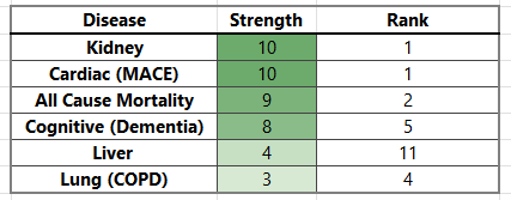
Cystatin C is a protein found in the blood measuring kidney function. It is not commonly monitored[1]. However, our models found Cystatin C in the top predictive biomarkers for every disease analyzed.
Below are the six diseases where Cystatin C was a top predictor, ordered by strength of association. The “Rank” column shows where on the list Cystatin C ranks in comparison to the other biomarkers.
Lipoprotein(a) is not predictive of any major diseases on our list.
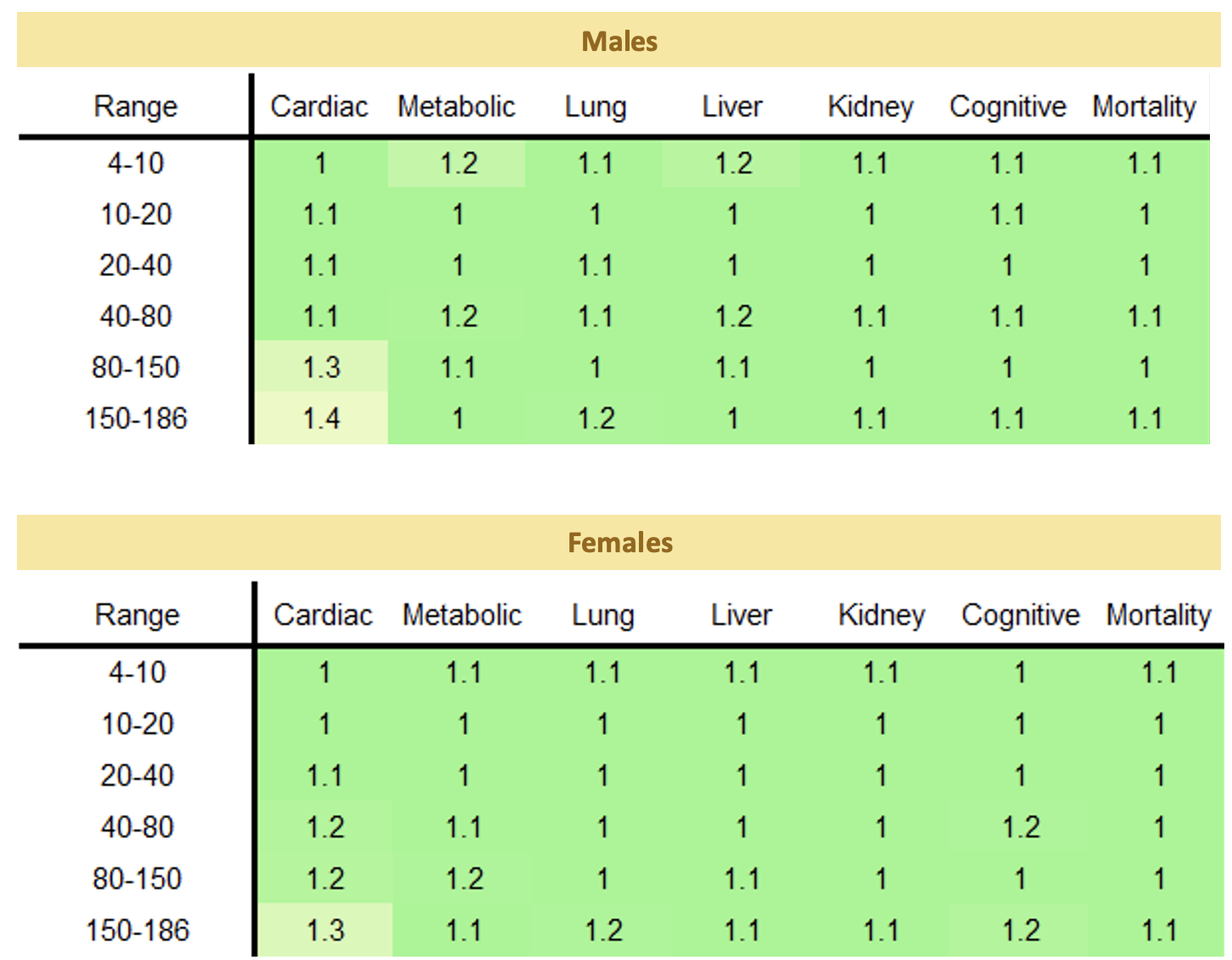
Lipoprotein(a) did not emerge as a top predictor for any disease on our list - despite being heavily monitored and a recommended test by physicians. In fact, our models found it to be especially unpredictive of all diseases, as shown in the table of risk multipliers below. Only cardiac (MACE) had an association with the highest values of Lipoprotein (a) but was modest in comparison with the associations of other biomarkers.
Quitting smoking leads to substantial risk reduction.
Smoking places enormous strains on the body in many ways including the impairment of cardiovascular and lung functions. It is never too late to quit using tobacco. The sooner a person quits smoking, the greater the individual reduction in cancer and other diseases.
Our initial findings are consistent with the literature from the American Cancer Society How to Quit Using Tobacco report[2]. We found substantial improvements in COPD and lung cancer risks after two years of quitting despite the “smoke pack” history. Reductions in the first years were strong across both COPD and lung cancer. The more packs per year history, the more opportunity for risk multiplier improvements.
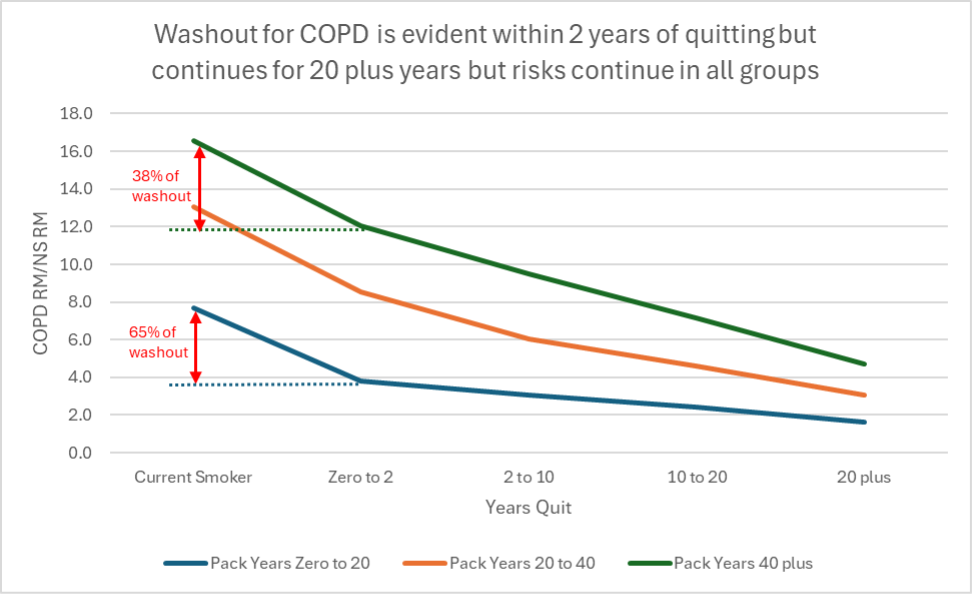
We found smokers who quit had risk multiplier improvements in COPD and lung cancer ranging from 23% to 51% in the first two years of quitting, and up to 83% reduction in the risk multiplier after 20 years. In comparison, the charts and graphs below show a non-smoker has a risk multiplier value of 0.27 for lung cancer and 0.38 for COPD.
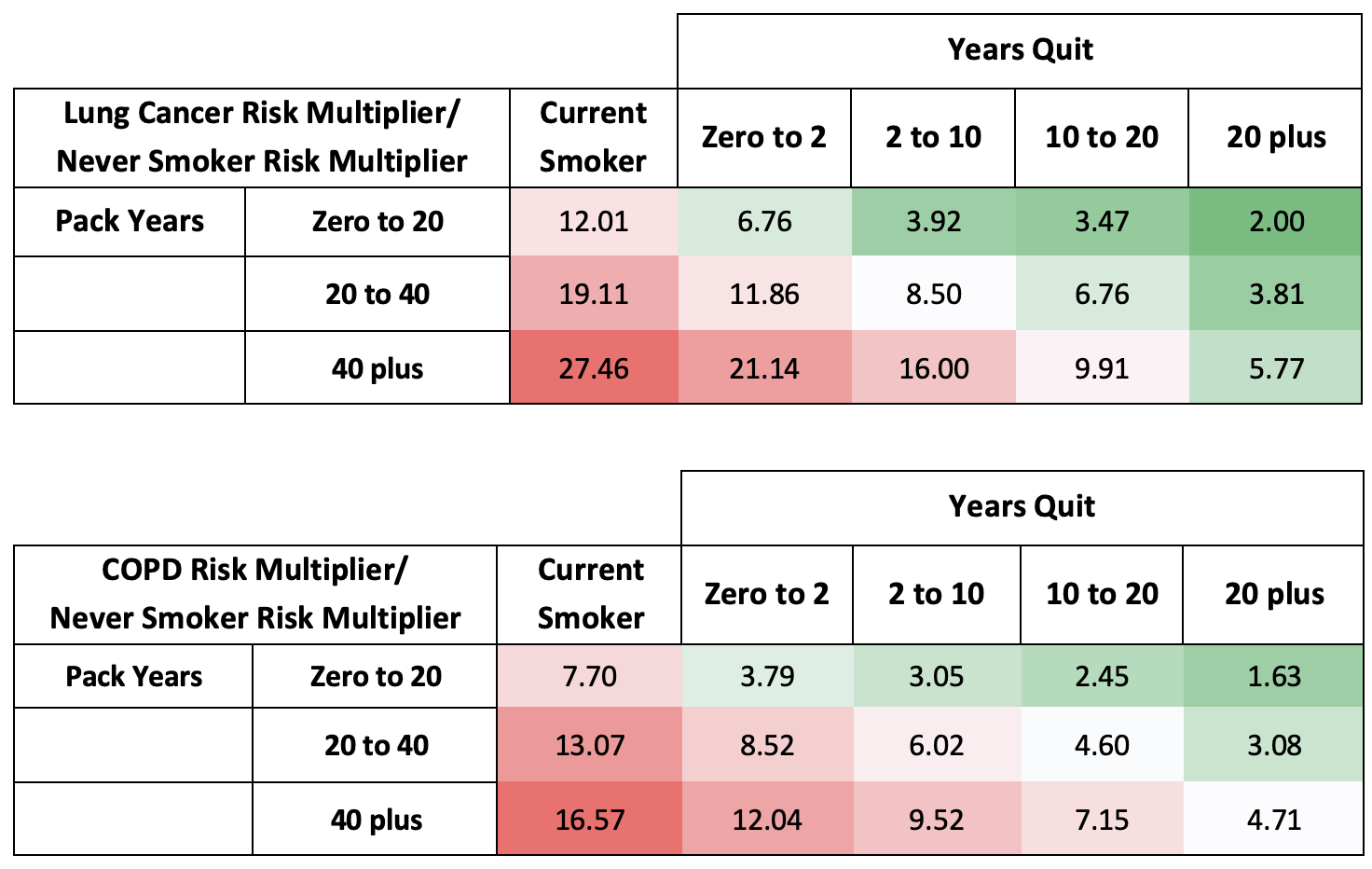
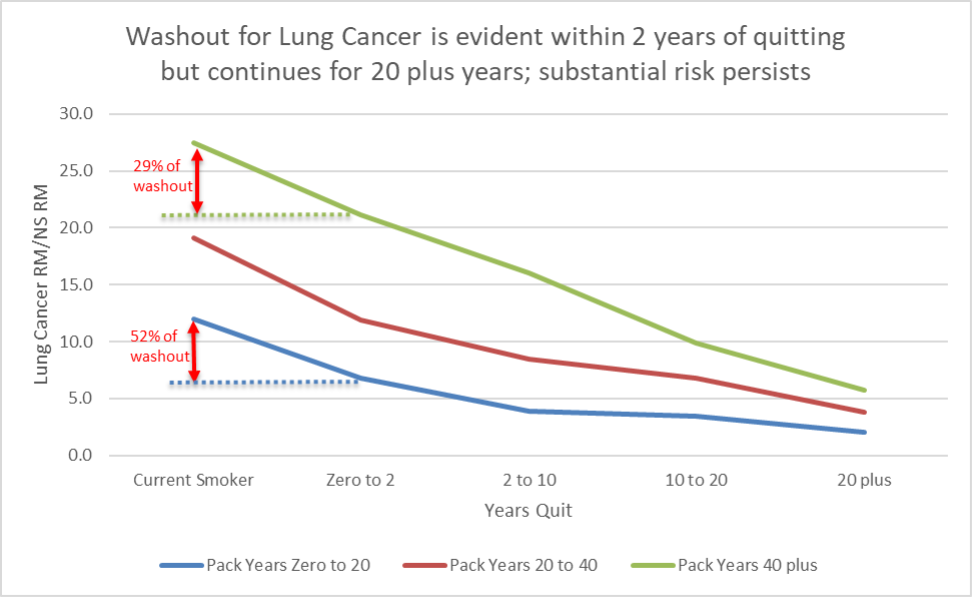
When comparing smokers to “never smokers” the early washout (resolution of the negative impacts of smoking) in the first two years is very strong for the lighter smoking history.
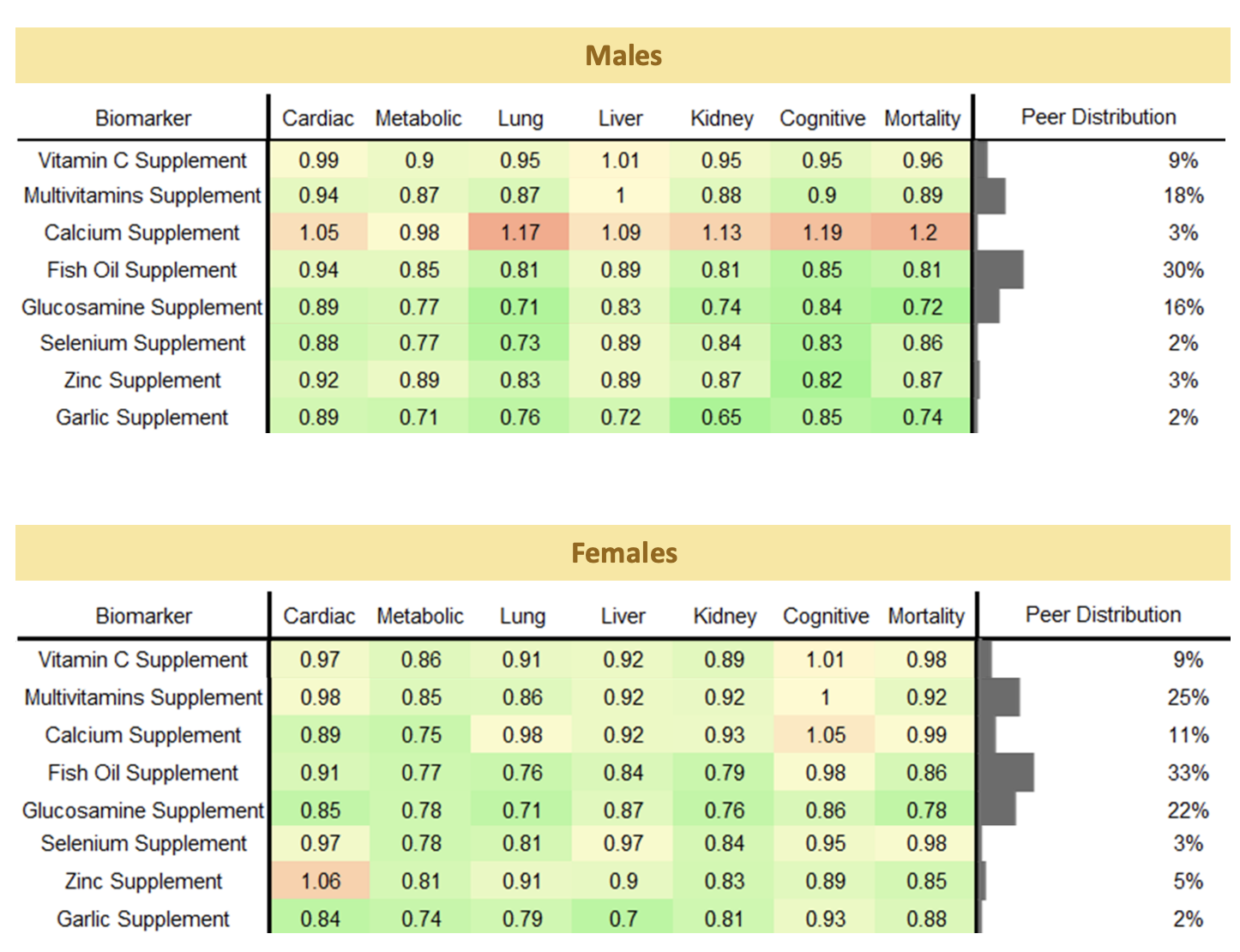
Nutraceuticals correlate with risk multipliers.
During the UK Biobank research we examined correlations of reported uses of several products. Our research is ongoing regarding these products and their impact on specific disease outcomes. Below are early results of correlations and risk multipliers for several products and the categories in this guide. We continue to refine this work and will report additional findings soon.
Nutraceuticals are the formulation of nutrients directed toward prevention and treatment of diseases (i.e. anemia, vitamin deficiencies), in addition to diet supplementation offering purported preventive health care choices for consumers. While the effects of many of these products on health and disease remain unclear, ongoing and future research will further shed light on their benefits and risks. Generally, nutraceuticals are not involved in clinical trials and approved by the FDA for statements related to improved health. For a comprehensive review please reference Nutrients, 2022 Nov 3;14(21):4637. https://www.mdpi.com/2072-6643/14/21/4637
[1] Cleveland Clinic. 2022. “Blood Tests: Types, Results & How They Work.” Cleveland Clinic. December 6, 2022. https://my.clevelandclinic.org/health/diagnostics/24508-blood-tests.
[2] www.cancer.org/content/dam/CRC/PDF/Public/9545.00.pdf